Is this the model to follow?
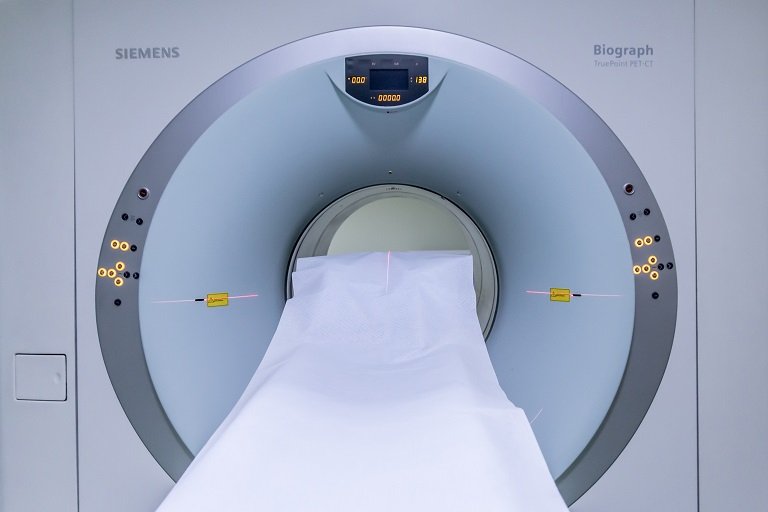
Community oncology clinics are closing or being acquired by hospitals at a swift pace and they are looking hard at the reasons why that’s the case, what makes sense financially and how it impacts the patient. It was argued that the site of care matters a lot and should be kept in the community setting – for the healthcare system in general and also for patients on an individual level. It has been noted that changing the site of care from low-cost physician offices to higher-cost hospital outpatient settings is one of the key cost drivers in cancer care. Reimbursement is much higher when the care is delivered in a hospital outpatient setting, rather than a physician’s office.
When a patient was told that her doctor was becoming part of a hospital system and her appointments would be at a facility 30 miles away she panicked. She was worried about the practical matter of how she would get to her appointments and how much extra time she would be spending in transit. She also worried about losing the close relationship with her clinic staff and how much more it was going to cost in a hospital outpatient setting where copays and out of pocket expenses are much higher. And what about cancers that are physically very painful or patients who are experiencing lots of complications – is asking them to travel long distances to receive care ok?
The medical profession must promote justice in the health care system, including the fair distribution of healthcare resources. Physicians should work actively to eliminate discrimination in health care, whether based on race, gender, socioeconomic status, ethnicity, religion, or any other social category. Patients should be cared for in the place where they will receive the best care at a fair price. They deserve the ability to get care in their community at a price they can afford.